Point of Care Microfluidics
SMART SYSTEMS TO DIAGNOSE ACUTE MYOCARDIAL INFARCTION.
2009 - 11
Acute Myocardial infarction (AMI), commonly known as a heart attack, is the interruption of the blood supply to a part of the heart, causing some cells to die.
Commonly caused by occlusions (blockages) to the coronary artery, the resulting ischemia (restriction in blood supply) and oxygen shortage can if left untreated for sufficient time periods cause damage or death (infarction) or heart muscle tissues (myocardium).
Classical symptoms include sudden chest pain (radiating to the left arm or left side of the neck), shortness of breath, nausea, vomiting, and anxiety, however over a quarter of AMI’s are silent, without chest pains or other symptoms.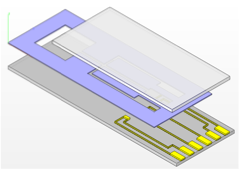
As with any heart attack, emergency medical treatment should be sought as soon as possible, since prompt protection from an external defibrillator can minimize the effects of primary ventricular fibrillation, which occurs in around 10% of AMI’s during the first hours of symptoms, with incidence peeking between 20 and 50 minutes after attack.
Risk factors for AMI’s include:-
•Previous Cardiovascular Disease (Angina / Stroke)
•Age – increasing likelihood for men (+40) and women (+50)
•Tobacco Smoking,
•High levels of lipids e.g. Triglicerides, and Low Density Lipoproteins (LDL Cholesterol) in the blood
•Low levels of high-density lipoprotein (HDL Cholesterol) in the blood.
•Diabetes,
•High blood pressure,
•Obesity,
•Chronic Stress,
•Excessive consumption of alcohol,
•Drug abuse (cocaine and methamphetamine).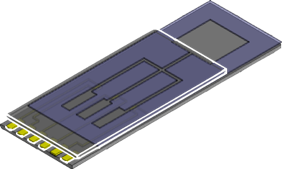
Immediate treatment for suspected AMI includes Oxygen, Asprin and glyceryl trinitrate (nitroglycerine). Additionally pain relief in the form of morphine sulphate is also used.
AMI Protein Markers
Cardiac markers or cardiac enzymes are proteins that leak out of injured myocardial cells through their damaged cell membranes into the bloodstream. Until the 1980s, the enzymes SGOT and LDH were used to assess cardiac injury. Currently, the markers most widely used in detection of AMI are of the MB subtype of the enzyme creatine kinase and cardiac troponins T & I and as these are more specific for AM injury.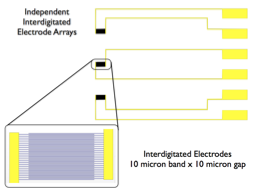
The cardiac troponins T and I are released within 4–6 hours of an AMI and remain elevated for up to 2 weeks and have nearly complete tissue specificity and are now the preferred markers for assessing myocardial damage.
The diagnosis of myocardial infarction requires two out of three components (history, ECG, and enzymes). When damage to the heart occurs, levels of cardiac markers rise over time, which is why blood tests for them are taken over a 24-hour period. Because these enzyme levels are not elevated immediately following a heart attack, patients presenting with chest pain are generally treated with the assumption that a myocardial infarction has occurred and then evaluated for a more precise diagnosis.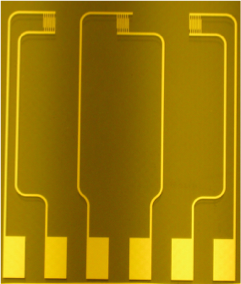
Aims of Project
•Development of a portable, low cost assay instrument to replace the clinical biochemistry lab approach to AMI assay.
•Use microfluidics to facilitate sample pretreatment, mixing, separation and transport serum from sampling site to analysis / assay.
•Use Impedance spectroscopy to measure enzyme binding related to concentrations / presence of AMI markers.
•Determine sensitivity levels required for AMI markers.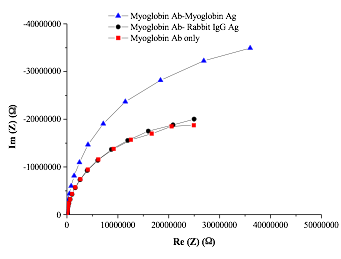
•Use micro-needles to instigate sub-dermal sampling.
•Develop low-cost impedance measurement instrument.
•Investigate / minimize interference effects of AMI markers.
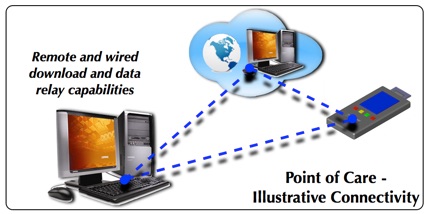
•Develop wireless communications network to relay data from sensor instrument to remote data station
(dumb terminal or data processing/monitoring)